
What Is Hospital Discharge?
Hospital discharge is the process of leaving hospital after a dedicated treatment when hospital staff decides a person no longer needs to stay and receive inpatient care. Being discharged includes practical steps such as receiving your discharge letter, understanding your medicines, arranging transport and knowing what support services people may need at home. To keep the discharge safe, timely and planned, with the right information, medicines, equipment, transport and follow-up support arranged before or soon after you leave hospital, many hospitals have a discharge planner.
A discharge planner is a healthcare or care coordination professional who supports safe hospital discharge. Discharge planners work with hospital teams, patients, families, carers, GPs, community services and social care teams to arrange the practical support needed after discharge. This may include medicines, equipment, transport, reablement care, home care, care home placement or follow-up appointments. Their role is especially important for complex discharge, where a patient needs ongoing health or social care support after leaving the hospital.
The Discharge Plan: Your Post-Hospital Roadmap
Leaving the hospital can feel like a relief, but it can also feel like standing at the edge of a doorway with no idea what waits on the other side. One moment, everything is structured: ward rounds, nurses, call bells, medication times, meals, observations, scans, conversations in corridors. Then suddenly, the question becomes: “Are you ready to go home?” And even when the answer is yes, another quieter question often follows: “But what happens now?”
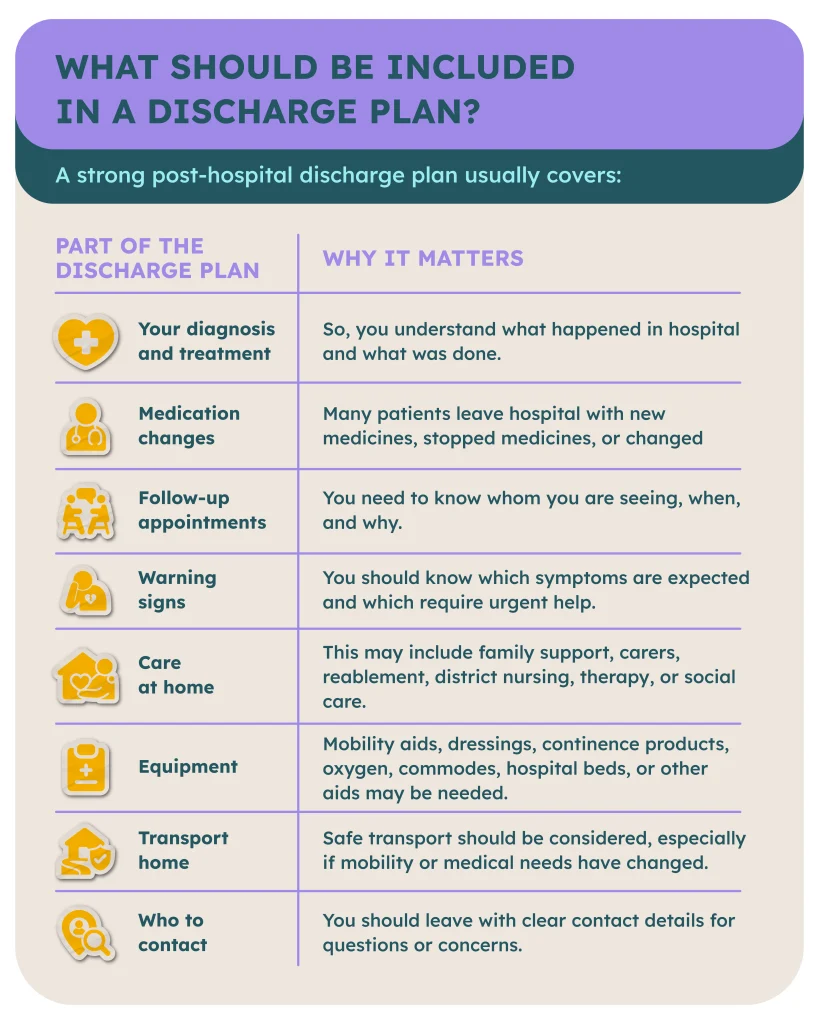
That is where the discharge plan comes in. A discharge plan is your post-hospital roadmap. It explains what needs to happen after you leave the hospital so your recovery does not feel like guesswork. It should help you understand your medicines, follow-up appointments, warning signs, care needs, equipment, transport, and who to contact if something does not feel right. At its best, a discharge plan is a bridge between the safety of the hospital and the uncertainty of home.
Why Effective Discharge Planning Matters
A hospital bed is not home. It is not where most people want to recover, rebuild their confidence, or return to themselves. Once people no longer need hospital care, home or a community setting, such as a care home, is often the best place to continue recovery. But discharge delays remain a real problem for many patients.
A good discharge plan helps answer the questions that matter most:
Will I be safe?
Who will help me?
What should I take?
What should I avoid?
What happens if I get worse?
Who is responsible for the next step?
Because recovery does not begin when the hospital doors close behind you. Recovery begins when you know what comes next.
Your Rights as a Family During Discharge
Often, hospital discharges are taken as something that simply happens to a person and their family. The ongoing discharge needs to be planned, explained, coordinated, and well executed through clear care plans, with the right care and support, ongoing support, and, where needed, rehabilitation support arranged before the person leaves the hospital. Usually, the hospital discharge team works with the person/patient, family, carers, NHS services, and the local authority to ensure the move from hospital to the person’s own home, an intermediate care service, or a supported living setting feels safe for the person.
Right to be Involved in Discharge Planning
If you are a family member or an unpaid carer who will be supporting the person after hospital, you should be involved in discharge planning where appropriate. This matters because families often know the reality behind the clinical notes. You know whether there are stairs at home. You know whether the bathroom is accessible. You know whether the person usually eats properly, remembers medication, becomes confused at night, or needs help getting out of bed.
Discharge planning should not be reduced to a rushed conversation at the end of a hospital stay. It should involve bespoke ongoing care and reablement care that fits the person’s needs. In personal terms, this means you can say: ”I am part of the care after discharge, so I need to be included in the discharge planning conversation.” You can ask who the named discharge coordinator or discharge planner is, what support has been arranged, whether a home assessment is needed, whether mental capacity has been considered if the person cannot make or communicate decisions, and whether the discharge plan reflects what the family can realistically provide.
Right to Receive Clear Information
A safe discharge depends on clear information. Families should not be left trying to decode medical language, guess medication changes, or piece together the plan from rushed conversations at the ward desk.
Before discharge, families and carers should ask for clear answers to questions such as:
- What has changed medically?
- What medicines should be taken, stopped or changed?
- What follow-up appointments are planned?
- What warning signs should we watch for?
- Who is responsible for care after discharge?
- What support is actually in place?
- Is intermediate care needed?
- Is there a rehabilitation plan?
A discharge plan should feel like a roadmap, not a riddle. It should help everyone understand what happens next, who is responsible, and what to do if the person’s needs change.
Right to a Carer’s Assessment Under the Care Act 2014
If you are going to provide unpaid care for an adult after hospital discharge, you may have the right to a carer’s assessment from the local authority.
Under the Care Act 2014 in England, carers have legal rights to assessment and support. The Health and Care Act also sits within the wider legal and policy landscape that shapes how NHS services, integrated care systems and local partners work together on health, social care and discharge. In practical terms, families should not be expected to provide unlimited care and support without their own needs being considered. A carer’s assessment looks at how caring affects you. It can consider your health, emotional wellbeing, work, education, family life, finances, ability to continue caring, and whether you are willing and able to provide the level of care being discussed. This matters when the discharge plan depends on you providing ongoing support or making sure the person can remain safely in their own home.
This is an important point: You are not automatically responsible for providing care just because you are family.
You can love someone deeply and still say:
- “I need support.”
- “I cannot safely provide that level of care.”
- “I am willing to help, but I cannot do everything.”
- “I would like a carer’s assessment before this plan depends on me.”

Right to Complain or Appeal if Discharge Feels Unsafe
If you feel the discharge is unsafe, you can speak up.
You may not be able to “appeal” hospital discharge in the same simple way as appealing a benefits decision, but you can challenge the plan, ask for it to be reviewed, request escalation, and make a complaint if you believe the discharge is unsafe or poorly handled.
You can ask to speak to:
- the nurse in charge
- the ward manager
- the discharge planner or discharge coordinator
- healthcare professionals
- the consultant or medical team
- the hospital social work team
- PALS
- the safeguarding team, if there is a serious risk of harm
- or the local authority adult social care team.
Types of Post-Discharge Care Available
Leaving the hospital is not always the end of care. For many people, it is the beginning of a new stage of recovery.
After discharge, the right type of care can help someone rebuild strength, regain confidence, manage medication, reduce the risk of readmission and return to daily life with dignity. Post-discharge care may involve NHS teams, council-funded social care, private providers, voluntary organisations, family carers, or a mixture of different health and social care services. The goal is simple but deeply important: to make sure the person is discharged safely and has the right support plan in place to support recovery.
Home Care
For many people, the best place to recover is at home. Home care can help someone return to familiar surroundings while still receiving practical ongoing support. It may include help with washing, dressing, meals, medication prompts, mobility, continence care, companionship, or support getting in and out of bed.
Home care may be arranged through NHS or council pathways, local care agencies, private care providers, or family-funded arrangements. The NHS explains that care after a hospital stay may include support after discharge, care at home, and help with recovery after illness, injury, or a fall.
In some cases, home care may also include short-term clinical support during recovery. This can involve visiting nurses, physical therapists and occupational therapists who provide medically necessary care at home after a hospital stay. For example, a visiting nurse may help with wound care, injections, medication management or monitoring symptoms, while a physical therapist may help rebuild strength, balance and mobility. An occupational therapist may assess how safely someone can manage daily activities such as washing, dressing, cooking or moving around their home.
Community Transitional Services
Community transitional services can also include short-term, intensive community programmes designed to help someone rebuild independence after a profound health shift or mental health event. This might follow a stroke, major surgery, serious infection, fall, long hospital stay, sudden loss of mobility, crisis in mental health, or a period where confidence and daily functioning have been deeply affected.
These services are not just about “checking in”. They are active recovery services that help a person relearn routines, regain confidence and gradually return to everyday life. Support may come from nurses, physiotherapists, occupational therapists, mental health practitioners, social workers, reablement workers or other health and social care professionals. Together, they may help with mobility, personal care, medication routines, emotional stability, home safety, daily living skills and confidence in the community.
Private Care
Private care is care arranged and paid for by the person or family, rather than fully funded by the NHS or local authority. For some families, private care offers flexibility, speed or additional choice. It may be used when someone does not qualify for funded care, while waiting for assessments, or when the family wants extra support beyond what statutory services provide.
Unique Community Services also offers private care for people who require complex care, delivered through specialist support from highly trained support workers and an in-house therapy team. What do we offer?
- Home care and support (domiciliary care, 24/7 care, personal care, respite care, live-in care, night care, housekeeping, transitional support and recovery care).
- Specialist care (Dementia, palliative, end-of-life, post-operative care, Alzheimer’s support, arthritis and mobility support, physical disability support, physical injuries support, learning disability support, stroke care, neurological support, reablement services and more).
- Healthcare (Diabetes care, catheter support, wound management, stoma support, feeding support, and vital signs monitoring).
To see more of how we can support you with private care, please click here.
Residential Care
Under residential care, we mean nursing homes, residential care homes, step-down beds, rehabilitation or respite settings, or other community-based placements. The most important thing is that people be discharged to the best place for them to continue their recovery in a safe, appropriate and timely way.
Residential care may be short-term or long-term. In many cases, the first step after the hospital should not be a rushed permanent decision. The discharge-to-assess approach is designed to allow longer-term needs to be assessed once the person has reached a more stable point in recovery. Residential care should be part of a clear support plan, with involvement from the person, family, carers, local services, NHS teams and social care professionals. Where the person has complex health needs, NHS continuing healthcare may need to be considered.
Before you make the right decision with and about your loved one, learn more about the Benefits of Choosing Private Home Care Over Institutional Care.
How to Prepare for Discharge (Practical Checklist)
Hospital discharge can feel overwhelming, especially when everything seems to happen quickly. One moment your loved one is being cared for on the ward, and the next you are being asked to think about medicines, transport, equipment, follow-up appointments and care at home. But preparation can make discharge feel less frightening. Use this checklist before discharge, on discharge day, and after discharge to help make the transition home, to intermediate care, or to another care setting feel safer and more organised.
Before Discharge: Questions to Ask and Things to Confirm
Before your loved one leaves the hospital, ask the hospital discharge team to explain the discharge plan clearly. Do not be afraid to ask the same question more than once. Discharge conversations can be emotional, and it is easy to miss important details.
- Can I have a written copy of the discharge plan and care arrangements?
- What is the expected discharge date, and could it change?
- Where is the person going after hospital care: home, care home, intermediate care or rehabilitation?
- Has the home environment been checked for safety?
- What equipment is needed, and will it arrive before the person gets home?
- What care services, community nurses or therapists will be involved?
- Will the person need ongoing support after any short-term care ends?
- Does the local authority need to assess care needs?
- Is a carer’s assessment needed for family members providing care?
- Are there any concerns about mental capacity or decision-making?
- What medicines should be taken, changed or stopped?
- Have follow-up appointments been booked?
- What warning signs should we watch for?
- Who should we contact if symptoms worsen or the care plan breaks down?
- Has suitable transport home been arranged?
On Discharge Day: What to Check Before Leaving the Ward
Discharge day can be busy and emotional. Families may feel relieved, anxious, rushed, or unsure whether everything is ready. It is worth pausing before leaving the ward to check the essentials. This is the moment to make sure the plan is not just written down, but actually workable.
- Has all their medication been supplied, or where and when should it be collected?
- Can someone clearly explain any medication changes to me?
- Do they have suitable clothes, shoes, mobility aids and personal items?
- Is their transport ready and suitable for their needs?
- Has any equipment they need at home arrived, or is delivery confirmed?
- Has their first contact for care, nursing, therapy, or recovery been arranged?
- Can I have the key contact details for the hospital, GP, community team or social care team?
- What should I do if they feel worse later today or overnight?
- Can you explain any wounds, dressings, catheters, feeding tubes, oxygen or other clinical needs?
- Can they safely get from the hospital to their home or next care setting?
- Do I, or any other family members or carers, need training before they leave?
- Does everyone understand the support plan?
- If something feels unsafe, can the discharge be paused and reviewed before they leave?
After Discharge: What to Watch, Track and Follow Up
The first few days after discharge can be the most uncertain. The person may be relieved to be home, but also tired, weak, emotional, confused or less independent than expected. This is normal for many people, but it is also the time to watch carefully. A discharge plan should continue to support recovery after the hospital doors close. If the plan does not work in real life, it should be reviewed.
- Have I booked or confirmed GP, hospital, therapy or community follow-up appointments?
- Am I watching for the warning signs the hospital explained?
- Am I keeping a record of falls, missed medications, worsening symptoms, or care gaps?
- Are carers, nurses, therapists or local services arriving as planned?
- Do I know who to contact if symptoms worsen?
- Is the current support plan enough for the person to cope safely?
- Do I need to ask for more care, social care support or a review?
- Is specialist support needed for dementia, mental health, stroke recovery, mobility, wounds, continence, nutrition or palliative care?
- Are family members and carers informed and coping?
- Do I, or another family carer, need to request a carer’s assessment?
- If the discharge feels unsafe, have I raised concerns immediately with the GP, community team, hospital, adult social care or PALS?
Working With Multidisciplinary Teams (MDTs) After Discharge
Originally, working with therapists helps strengthen people’s life skills and support recovery in their homes. Having PBS practicioners, occupational therapists, speech and language therapists, and multimedia specialists is the ideal scenario. When the same team is an in-house multidisciplinary team with a human-centric approach and does a comprehensive needs assessment, people ultimately feel more confident and joyful about their specific recovery plan. Having a trusted team of specialists also makes the whole healing journey smoother for families.
Our in-house therapists are accredited in PROACT-SCIPr-UK® and Positive Behaviour Support (PBS). The main goal is to support people in becoming active citizens and integral parts of their own communities. Why choose us?
- Our therapy team makes shared-decision making
- They provide holistic support combined with clinical care where needed
- They follow consistent and structured routines tailored for each person’s individual needs
- Our therapists create conditions for positive risk-taking, followed by visible positive outcomes
- They build trusting relationships with the person they serve, their family or any other stakeholders involved in the support.
Clinical Care After Hospital Discharge with Unique Community Services
When our care teams create support plans for the people we serve, the care plans reflect the whole person, their health and social needs, routines, preferences, and life goals. The care plan is built with the person, their family and health professionals. What to expect from our clinical care teams?
- Highly skilled clinical team in evidence-based practices, PROACT-SCIPr-UK® and Positive Behaviour Support (PBS).
- Clinical support that happens smoothly within everyday routines.
- Focus not just on safe care, but on a better life.
How can we support you?
- Personal care and daily living support
- Assessment and management of the condition
- Coordinated care
- Social and emotional support
- Safe treatment and medication administration
- Pain monitoring and relief support
- Specialist wound care and health promotion
- Well-coordinated hospital transitions
Meet Elijah.
Whether you need long-term complex care, are planning a transition, are seeking reliable care partnerships, or are exploring bespoke support options, our team is here to help.
Contact us today to start building solutions together.
